Heart Attack Is Not Cardiac Arrest: When Confusing Terms Can Cost Lives
In the popular imagination, the terms “heart attack” and “cardiac arrest” often circulate as if they were the same thing. In news reports, someone “had a cardiac arrest” when, in fact, they suffered a heart attack. In everyday conversations, the words get mixed up. In biology, however, they represent radically different failures within the same system — and this semantic confusion can delay decisions that must be made within minutes.
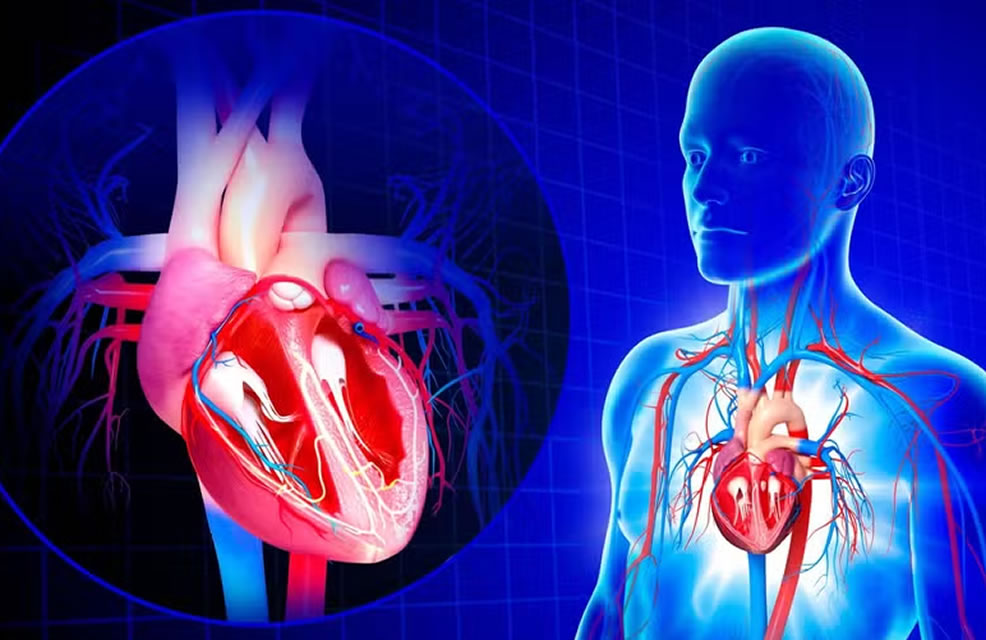
The human body works like an extraordinarily delicate machine, supported by two inseparable pillars: efficient circulation and precise electrical control. The heart is not only a muscular pump; it is also a living electrical circuit. When blood flow fails, we have a hydraulic problem. When electrical rhythm collapses, we have an energy problem. When both fail at the same time, life enters immediate danger.
Understanding the difference between a heart attack and cardiac arrest is not a technical detail reserved for doctors. It is survival literacy. It is knowing what is happening while there is still time to act.
A heart attack: when the heart suffers while you’re awake
The technical term is acute myocardial infarction. The myocardium is the heart muscle. An infarction means tissue death caused by lack of oxygen.
In most cases, it starts in one of the coronary arteries — vessels responsible for nourishing the heart itself. Over the years, plaques of fat, cholesterol, and inflammatory cells can build up along the artery walls. This process, called atherosclerosis, is silent and progressive.
At some point, the plaque can rupture. The body interprets the rupture as an injury and forms a clot. The problem is that this clot can completely block the artery.
The result is a supply crisis.
The heart keeps beating. The person is conscious. But part of the muscle begins to receive less oxygen. Pain arises because heart cells deprived of oxygen release inflammatory substances that stimulate local nerves.
The classic description is well known:
· pain or tightness in the center of the chest,
· a feeling of pressure or heaviness,
· radiation to the left arm, jaw, or back,
· cold sweat,
· nausea,
· a sense of impending doom.
But biology rarely respects classic descriptions.
Silent heart attacks and atypical presentations
In older adults, people with diabetes, and many women, a heart attack may not present as intense chest pain. It can appear as:
· sudden extreme fatigue,
· shortness of breath,
· abdominal pain,
· a vague, hard-to-explain malaise,
· dizziness.
In people with diabetes, for example, nerve changes can reduce the perception of pain. The heart is suffering — but the body doesn’t shout.
Regardless of how it appears, the internal process is the same: progressive ischemia (reduced blood flow) that can evolve into necrosis (irreversible tissue death) if circulation is not restored.
There’s a saying in cardiology: “time is muscle.”
The longer the artery remains blocked, the larger the area of muscle that dies.
A heart attack is therefore a biological time bomb.
There is time — short and precious — to intervene.
What truly saves lives in a heart attack
Unlike what many people imagine, the definitive treatment for a heart attack is not rest or a painkiller. It is restoring blood flow.
This can be done in two main ways:
· thrombolysis (medication that dissolves the clot),
· angioplasty (a procedure that opens the artery with a catheter and places a stent).
The earlier this happens, the greater the chance of preserving heart muscle.
That’s why emergency services insist: if you have suspicious chest pain, don’t wait for it to “go away.” Don’t drive yourself to the hospital. Call emergency services. Every minute matters.
Cardiac arrest: the sudden silence of the machine
If a heart attack is progressive suffering, cardiac arrest is abrupt collapse.
In cardiac arrest, the central problem is not necessarily a blocked artery. What fails is the heart’s ability to pump blood effectively.
The heart has its own electrical system. A small group of cells in the right atrium — the sinoatrial node — generates rhythmic electrical impulses. These impulses travel along specific pathways and coordinate muscular contraction.
When this system falls into chaos, severe arrhythmias appear.
The main causes of cardiac arrest include:
· ventricular fibrillation (the heart quivers chaotically),
· pulseless ventricular tachycardia,
· asystole (no electrical activity),
· pulseless electrical activity (there is electrical signal, but no effective contraction).
The result is immediate:
blood stops circulating.
The brain begins to suffer within seconds. Consciousness is lost almost instantly. After about 4 to 6 minutes without oxygen, the risk of permanent brain injury rises rapidly.
It’s not progressive pain.
It’s a sudden collapse.
How to recognize cardiac arrest
The main signs are:
· sudden loss of consciousness,
· no response,
· no normal breathing,
· no palpable pulse.
In the first moments, irregular, noisy breathing-like movements can occur, called “gasping.” This is not effective breathing. It is the nervous system trying to sustain life as the body collapses.
Here, there is no room for passive observation.
Cardiac arrest is an absolute emergency.
The only chance of reversal is immediate intervention with:
· cardiopulmonary resuscitation (CPR),
· defibrillation when indicated.
The defibrillator and the physics of life
Ventricular fibrillation is one of the most common causes of sudden cardiac arrest. In this state, the heart’s cells fire electrical impulses chaotically. There is no coordinated contraction.
A defibrillator does not “restart” the heart like in the movies. It delivers an electrical shock that momentarily interrupts all disorganized electrical activity, giving the sinoatrial node a chance to regain control.
It’s an electrical reset.
Every minute without defibrillation significantly reduces the chance of survival. In many countries, automated external defibrillators (AEDs) are available in airports, gyms, and shopping centers for exactly this reason: any trained person can use them.
The dangerous link between heart attack and cardiac arrest
A heart attack and cardiac arrest are not the same — but they can be connected.
A heart attack can trigger cardiac arrest by causing electrical instability in the injured muscle. Ischemic areas become electrically unstable and can generate fatal arrhythmias.
On the other hand:
· many cardiac arrests occur without a prior heart attack,
· many heart attacks do not progress to cardiac arrest when treated quickly.
This distinction completely changes the required response.
In a heart attack:
the goal is to restore blood flow.
In cardiac arrest:
the focus is to temporarily replace the heart’s function with chest compressions and restore electrical rhythm.
Confusing the two can delay critical decisions.
Sudden cardiac arrest in young people: a different phenomenon
While heart attacks are mainly associated with atherosclerosis in adults, cardiac arrest can occur in young people for other reasons:
· inherited cardiomyopathies,
· congenital electrical disorders,
· myocarditis (inflammation of the heart muscle),
· severe chest trauma,
· use of stimulant drugs.
In athletes, rare cases of sudden arrest during physical activity are often linked to pre-existing structural or electrical abnormalities.
This reinforces that cardiac arrest is not synonymous with “a blocked artery.”
Fluid mechanics and electricity: two interdependent systems
The heart depends simultaneously on:
1. Clean plumbing (unobstructed coronary arteries).
2. A functional electrical circuit.
If the hydraulic system fails, we get muscular suffering.
If the electrical system fails, we get immediate circulatory collapse.
Life depends on the balance between these two mechanisms.
It is biological engineering running continuously.
Risk factors: where prevention begins
A large share of heart attacks is associated with modifiable factors:
· smoking,
· high blood pressure,
· diabetes,
· high cholesterol,
· physical inactivity,
· obesity,
· chronic stress.
Cardiac arrest can occur as a consequence of these same conditions, but it can also result from genetic predispositions.
Cardiovascular prevention is, to a large extent, heart-attack prevention.
And preventing heart attacks indirectly reduces the risk of cardiac arrest.
The role of bystanders: acting can save lives
Studies show that bystander CPR doubles or triples survival chances in out-of-hospital cardiac arrest.
Chest compressions maintain minimal circulation to the brain and vital organs until specialized help arrives.
You don’t need technical perfection to save a life.
You need to act.
In suspected heart attacks, recognizing symptoms early and seeking immediate care also drastically changes the outcome.
A difference that changes destiny
In a heart attack, the person is usually awake, in pain, asking for help.
In cardiac arrest, the person collapses and loses consciousness.
In a heart attack, there is still circulation.
In cardiac arrest, there is no effective blood flow.
In a heart attack, time is critical.
In cardiac arrest, time is brutal.
Confusing the two means reducing the complexity of biology to a single label — and that simplification can cost minutes that determine survival.

The fragility of life in seconds
The heart is not just an emotional symbol. It is a muscular pump and a synchronized electrical circuit.
When it suffers, the body warns you.
When it stops, the body goes silent.
Knowing how to tell these two situations apart is understanding that life depends on both flow and rhythm.
Because, in the end, it’s not just about names.
It’s about recognizing what is happening while there is still a chance to intervene.
Important note
This content is educational and informative. It does not replace an in-person medical evaluation and must not be used for self-diagnosis. If you experience symptoms suggestive of a heart attack or suspect cardiac arrest, seek immediate medical care or call emergency services in your region.